
Nipple reconstruction surgery
Nipple reconstruction, also known as areola reconstruction, is typically undertaken after autologous reconstruction or implant reconstruction has taken place. It is a treatment which is best scheduled at least three or four months after reconstruction surgery so that the reconstructed breast has the necessary time to heal.
Nipple reconstruction surgery
Nipple reconstruction, also known as areola reconstruction, is typically undertaken after autologous reconstruction or implant reconstruction has taken place. It is a treatment which is best scheduled at least three or four months after reconstruction surgery so that the reconstructed breast has the necessary time to heal.
Frequently Asked Questions
Nipple reconstruction is sometimes known as areola reconstruction and is normally undergone following an autologous reconstruction or implant reconstruction. This procedure is normally scheduled three months or more after reconstruction surgery has taken place. This is to give the reconstructed breast enough time to heal.
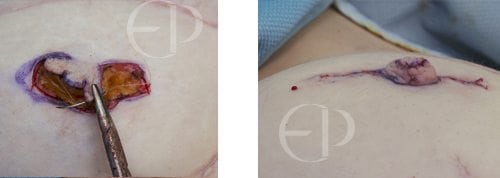
Nipple reconstruction is often needed after a mastectomy has taken place which involves the removal of the nipple and areola. A nipple reconstruction will recreate the darker coloured areola, along with the elevated nipple. Usually a technique using local skin flaps is used. The type of local skin flap which is used will be decided by the surgeon.
The decision to have a nipple reconstructed following an autologous reconstruction or implant reconstruction will come down to the patient’s personal choice. Elena will offer her advice through a series of examinations and consultations, talking patients through all the pre-surgery investigations which will be necessary.
Nipple reconstruction uses the skin surrounding the site which has been selected for nipple placement.
In the case of inverted nipples, these can be corrected easily with 2mm incisions around the nipple. Scars are nearly invisible in this case. Secondary adjustments to the reconstructed breast itself are sometimes needed, and these can be made at the same time as the nipple reconstruction operation. These secondary breast correction surgery adjustments can include lipofilling to the flap, helping to match volume and shape, as well as uplifts and contralateral reductions.
The local skin flaps which can be used in nipple reconstruction include the C-V flap, star flap and skate flap. The decision on which local skin flap to use will be influenced by the priority of minimising the risk of bleeding. When using a skin graft for the areola, some surgeons tattoo the grafted area in order to increase skin pigmentation.
Prior to the nipple reconstruction procedure, it is common for patients to refrain from drinking or eating for a window of six hours. An anaesthetist will be available to discuss the chosen mode of anaesthesia with the patient prior to them entering the operating room.
As with all surgical procedures, nipple reconstruction involves a small amount of risk. Although there is a small chance of them, potential complications include bleeding, loss of nipple sensation and the need for revision surgery to be carried out.
A very rare potential complication involves the nipple used in the reconstruction not receiving enough blood, causing some of it to die. In this instance, the dead tissue needs to be trimmed away and the nipple reconstructed. Another rare complication is for the nipple to flatten out too much. This problem can be addressed by the reconstruction and reinforcement of the nipple with a graft.
Nipple reconstruction patients typically wear a nipple shield for protection following the procedure. This can be kept on for a period of about three days. Stitches are usually removed around two weeks after the procedure, swelling then begins to flatten out. The nipple can feel tender for a week or so after the procedure.
Recovery rates can be dependent upon which other revisions are undertaken at the same time as the nipple reconstruction, as well as the areola graft’s location site. Medication can be prescribed in order to ease the discomfort felt during the recovery period. The majority of swelling and bruising should subside within two to three days after the procedure. Some scars might not disappear altogether, but most should fade to a large degree after a few months.
While a nipple cannot be reattached weeks later following its removal as part of a mastectomy, there is the potential for nipple sparing techniques to be used which preserve and reattach the nipple during the nipple reconstruction procedure. Nipple sparing mastectomies can be ideal for women with a tumour which does not involve the tissue or nipple beneath the areola; women who have not been diagnosed with advanced or inflammatory breast cancer which has a skin involvement; and women who have tumours with a clear area of cancer-free tissue surrounding them.
Elena is recognised internationally for her award-winning work in cosmetic surgery. She offers patients the benefits of an expert female consultant with an empathetic attitude and the choice of several UK locations; from London to Bristol and Sussex. With Breastclinik, you have access to cutting-edge techniques and a superb standard in aftercare.
The total cost of the surgery will be confirmed after the first consultation.
The cost includes the hospital, surgeon and anaesthetic fees. It also covers all post-operative visits. The initial consultation fee will be invoiced separately. The prices apply only at the time of publication and are subject to changes without notification.
Surgery costs from £2,995
Initial consultation fee £150
Surgery details
Anaesthetic: Local or General
Follow up: 1,4 weeks, 12 months
Recovery time: 1-2 Weeks
Surgical time: 1.5-2 Hours







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}